Occipital neuralgia is a condition that causes severe pain in the back of the head, often radiating towards the upper neck or the back of the eyes. This pain occurs when the occipital nerves, which begin in the spinal cord and then run in the muscles of the neck through the scalp, are inflamed or injured. It can feel like a sharp, jabbing electric shock in the back of the head and neck. At our center, understanding this pain and its impact on your life is the first step in our approach.

Occipital Nerve Decompression Migraine Surgery
Case 1
For those patients and others that are interested in seeing what migraine surgery actually looks like, here are some photos from one of my occipital neuralgia patients during her surgery. This woman had nearly daily headaches that had been not responded to treatment from multiple neurologists and pain management doctors. Following her surgery to date, she is free of all headache pain. All photos are displayed with full consent from the patient.
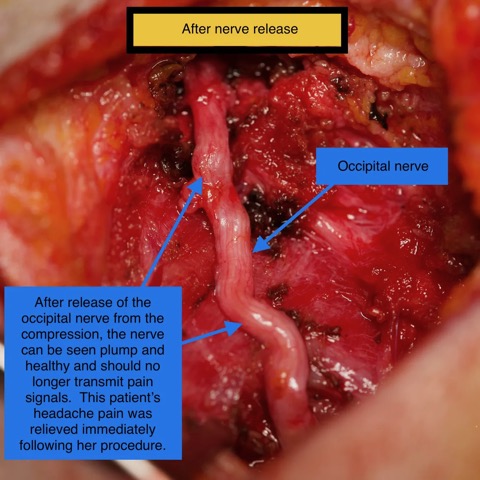
This patient is a very pleasant 40-year-old woman who has had 5 1/2 years of severe headaches. She has three children and a husband in graduate school and ad been unable to function to perform her day-to-day activities. She has seen multiple physicians and had multiple failed attempts at relief. She has seen a neurologist, headache specialist, and pain specialist. She has had MRIs and CT scans as well as MRA studies which have not shown anything wrong. She has tried multiple medications with no improvement. Her occipital nerve was clearly compressed and irritated, and once released from compression, she had immediate relief of her headache in the recovery room right after surgery.
Case 2
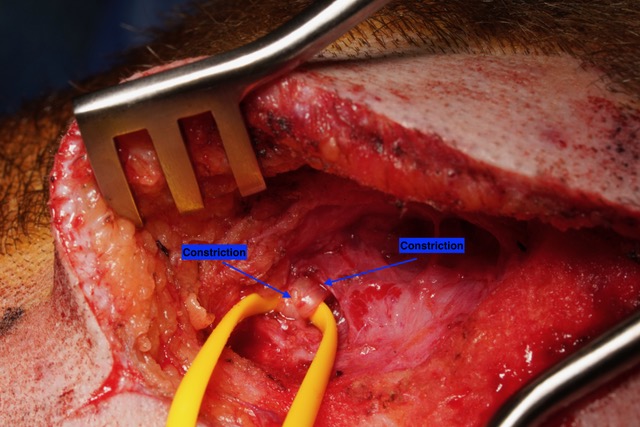
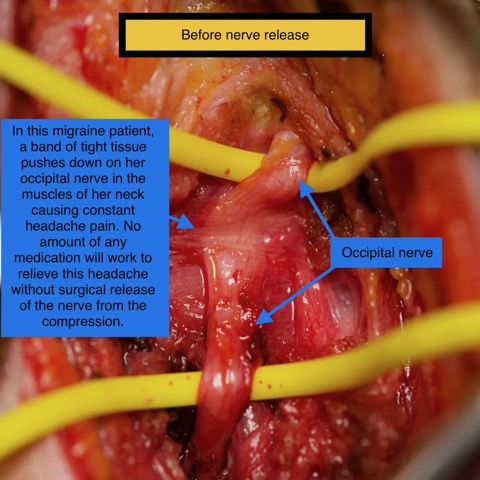
This photo shows the occipital nerve as it is first encountered during surgery. The nerve can be seen to be constricted by the surrounding muscle, causing irritation that is causing this patient’s migraine headache pain.
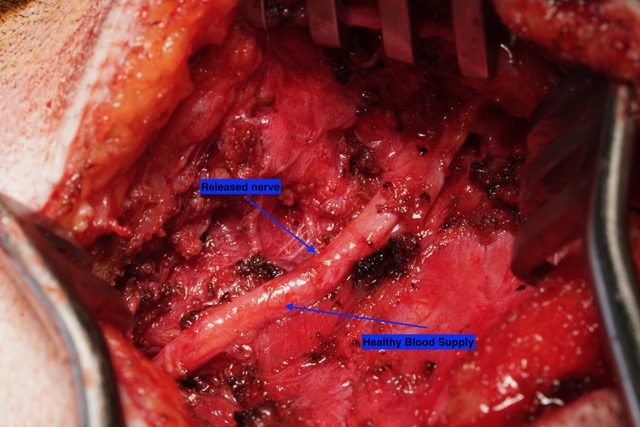
Following the release of the nerve, it can be seen here in this photo as plump and healthy, no longer compressed by the surrounding tissue. Healthy blood supply can now be seen around the nerve, as it appears more pink than white as the first photo shows.
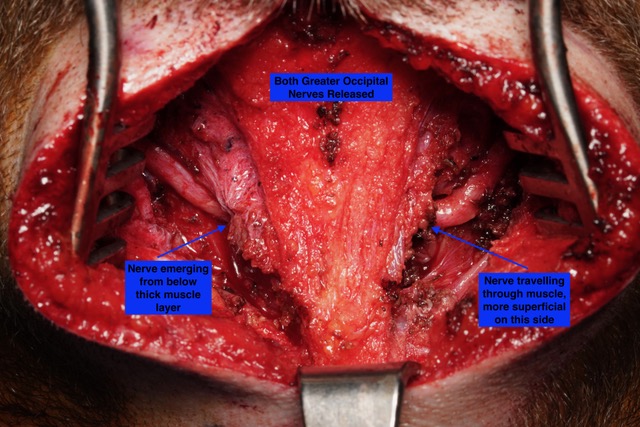
This photo shows both greater occipital nerves following nerve decompression. Each nerve has a different course. The one on the left emerges from more deep muscle, while the more superficial course of the nerve on the right can be seen. It is not unusual for each nerve to have a different course in the anatomy of the neck.
Case 3

This photo shows the pre-operative markings for this patient who is about to undergo migraine surgery for occipital neuralgia. IMPORTANTLY, THIS PATIENT CHOSE TO SHAVE HER ENTIRE HEAD, AND THIS IS NOT NECESSARY FOR THE OPERATION. The X at the top represents the occipital protuberance, and the midline marking shows the plane in which the incision will be made. The dots represent where the greater occipital nerve and third occipital nerve can be found, but the Xs toward the bottom of the photo are over the points where this patient felt a “Tinel” sign, or sensitivity to tapping on the third occipital nerve. The smaller, lower lines on each side and the dot in the middle of that line represent the incisions for the approach to the lesser occipital nerves, and the point at which we expect that nerve to be found, respectively. While it is not necessary to shave this region the head, this patient did so on her own the day before surgery.
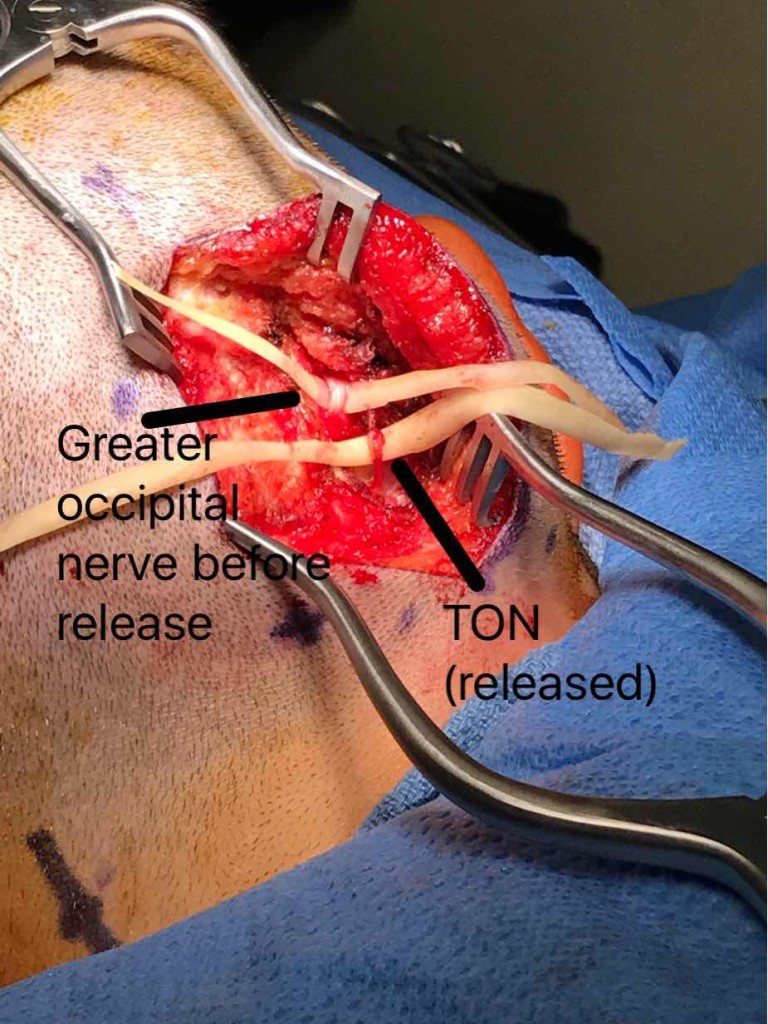
The photo shows the third occipital nerve (TON) in the lower portion of the incision. The greater occipital nerve is seen above it just as it was identified, constricted by the surrounding muscle and connective tissue. This migraine surgery incision is in the midline of the back of the patient’s head and upper neck.
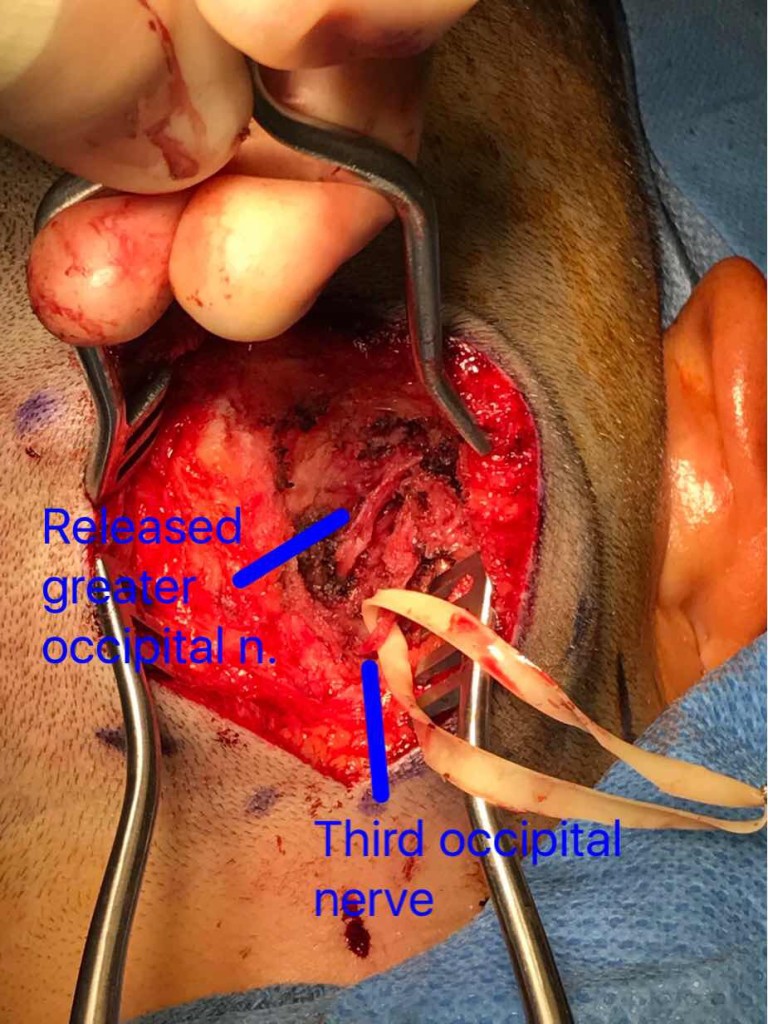
In this photo taken during migraine surgery for this same woman with a long history of occipital neuralgia, the greater occipital nerve can be seen now free of the surrounding constrictive structures, coursing from the deep tissue (splenius capitis muscle toward the middle of the photo) up toward the upper right hand corner of the frame, where it enters the looser subcutaneous space. The third occipital nerve, seen with a rubber loop around it, has also been freed but is associated with neuromatous tissue and was therefore subsequently cut. This woman found complete relief from her headaches immediately following this operation.

In this photo, the lesser occipital nerve has been dissected from the surrounding tissue. This nerve emerges from the posterior border of the sternocleidomastoid muscle. For reference, the top of this patient’s head is toward the right of the photo and the back of the ear can be seen toward the bottom of the photo.
Case 4
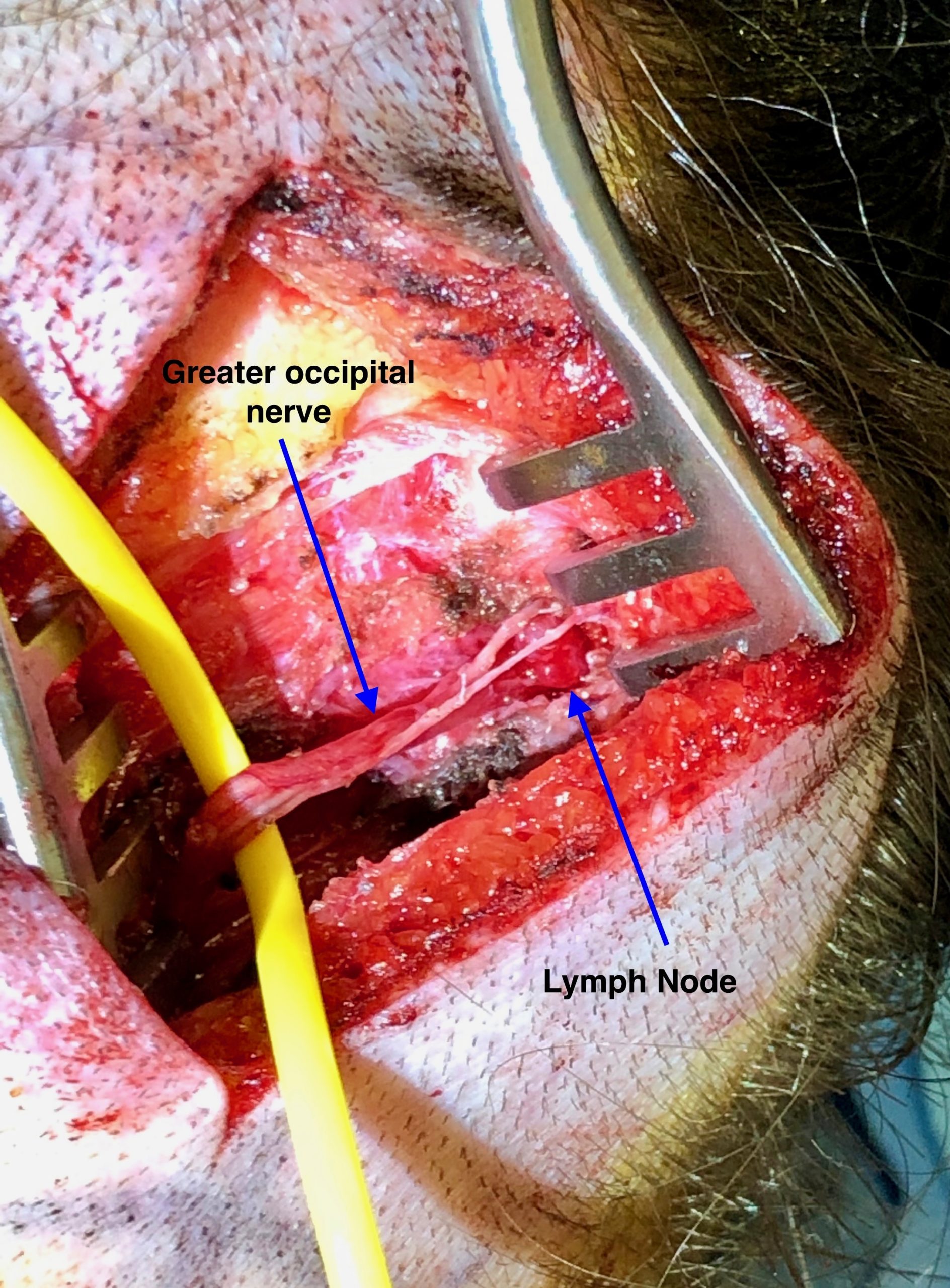
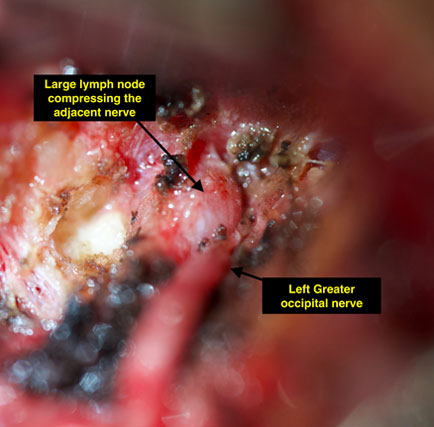
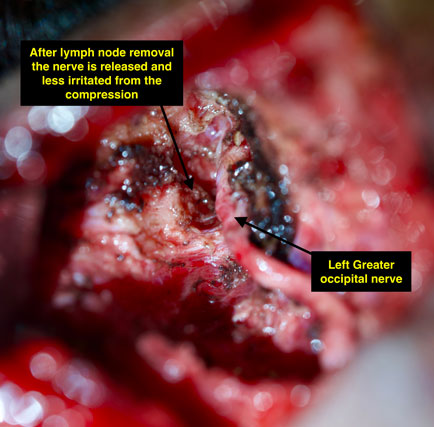
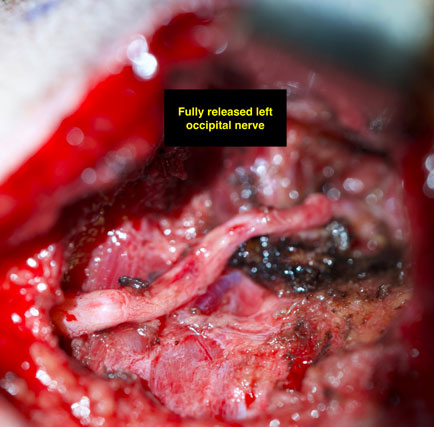
In this photo, a lymph node is found in the upper course of the greater occipital nerve, putting pressure on the nerve itself. This is another type of structure that can cause nerve compression and these lymph nodes are removed during nerve decompression surgery so that the occipital nerve can course more freely without excessive irritation and compression from surrounding structures.
Case 5
This patient suffered from complex and severely painful migraines for more than 15 years. She was unable to be productive as a computer programmer, and the severe pain from her headaches affected her professional and social life severely. She has been treated by multiple headache specialists (including neurologists and pain doctors) for many years without headache resolution.
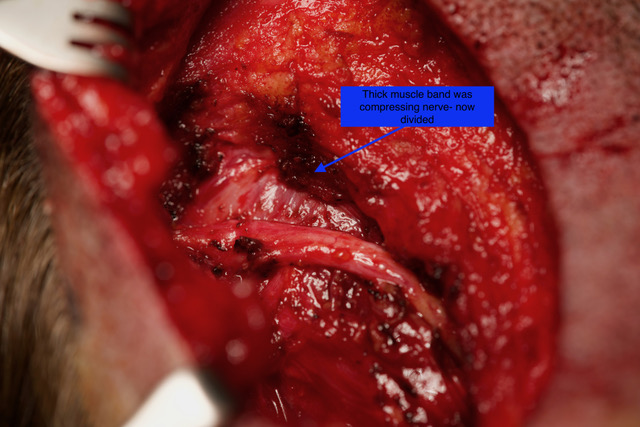
During her occipital nerve decompression, very interesting findings were noted. On the left, more painful side, this patient had a very thick muscle band, called the trapezius fascia, that was over 1cm thick and pushing right on her occipital nerve trunk. Recent research out of Harvard[1] has shown that patients with severe headaches often have much thicker trapezius fascia than normal. This patient demonstrates how release of this thick tissue removes the compressive irritation that produces migraine pain, as her discomfort was significantly improved immediately after surgery.
[1] Gfrerer, Lisa M.D., Ph.D.; Hansdorfer, Marek A. M.D.; Ortiz, Ricardo M.D.; Chartier, Christian; Nealon, Kassandra P. B.Sc.; Austen, William G. Jr. M.D. Muscle Fascia Changes in Patients with Occipital Neuralgia, Headache, or Migraine, Plastic and Reconstructive Surgery: January 2021 – Volume 147 – Issue 1 – p 176-180 doi: 10.1097/PRS.0000000000007484
Case 6
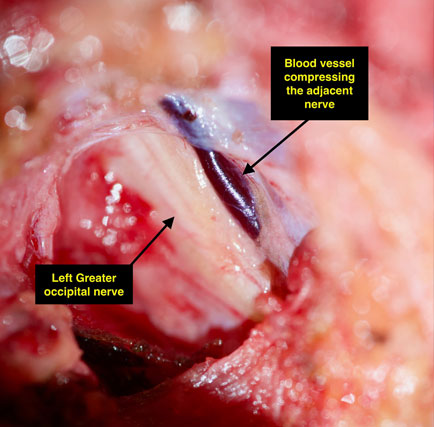
This very pleasant 39 year old nurse had headaches and migraine headaches since childhood. She used to be able to manage her headaches with Advil but they became progressively worse over time. Her pain became associated with blurry vision and nausea. Her occipital nerve release headache surgery revealed a blood vessel pushing on the nerve, as well as a lymph node pushing on the nerve. This irritation from these nearby structures was alleviated by her migraine surgery when the blood vessel and lymph node were removed. Following her surgery, she has been “amazed’ at the big difference in her headache pain and her personality, and reports being much happier overall. Her migraines, even less than one month out from surgery, are much less frequent and respond easily to medication. She has no more visual disturbances or nausea. Her symptoms should continue to improve further in the coming months.
What is Occipital Neuralgia?
Symptoms
The symptoms of occipital neuralgia are distinct and can often be debilitating. Patients typically experience:
- intense, sharp pain that can mimic the shock-like sensation of an electric shock.
- Pain on one or both sides of the head.
- Sensitivity to light.
- Tender scalp.
- Pain when moving the neck.
Recognizing these symptoms early can lead to more effective treatment options, including surgery for occipital neuralgia, which we expertly provide at our center.
Causes
The exact cause of occipital neuralgia can vary but typically involves the compression or irritation of the occipital nerves. Common causes include:
- Trauma to the back of the head.
- Neck tension or tight muscles.
- Prolonged periods of keeping the head in a downward and forward position.
- Blood vessels or lymph nodes compressing the nerve
Understanding these causes helps us tailor our approach to treating occipital neuralgia, ensuring that each patient receives personalized care.
Risk Factors
Certain factors may increase the risk of developing occipital neuralgia, including:
- Previous neck injuries.
- Chronic neck tension or tight muscles.
- Inflammatory diseases.
- Frequent prolonged posture that strains the neck and back of the head.
- Infections causing inflamed lymph nodes
Awareness of these risk factors is crucial for both prevention and early intervention, which can significantly improve outcomes for sufferers of this painful condition.
Occipital Decompression Surgery
At Migraine Surgery Specialty Center, we specialize in occipital decompression surgery—a procedure designed to relieve the pressure on the occipital nerves. This surgical approach is considered when other treatments have not provided sufficient relief. The procedure involves:
- Identifying and exposing the irritated occipital nerves.
- Carefully releasing any compressive elements, such as tight muscles or fibrous bands.
- Ensuring there is enough space around the nerves to prevent future compression.
Our experienced surgeons use the latest techniques and technology to perform occipital release surgery, offering hope and relief to those who have suffered prolonged pain.
FAQs
1. What is Occipital Nerve Decompression Surgery?
Occipital nerve decompression surgery, also known as occipital release surgery, is a procedure designed to alleviate the pain caused by occipital neuralgia. This condition results from the occipital nerves being compressed or irritated, often leading to severe headaches. During the surgery, our skilled surgeons carefully free the occipital nerves from any compressive tissues or abnormal muscle tensions, providing them with more space to heal and reducing the possibility of future compression.
2. How Successful is Occipital Release Surgery?
The success of occipital release surgery can vary based on several factors, including the patient’s specific condition and the extent of nerve compression. However, most of our patients experience significant relief from their symptoms post-surgery. Clinical studies and our own outcomes data suggest that a substantial percentage (up to 93%) of patients report a decrease in the frequency and intensity of their headaches, with many achieving lasting relief.
3. What is the Recovery Time for Occipital Nerve Surgery?
Recovery times can vary, but most of our patients begin to see improvements within a few weeks after their occipital neuralgia surgery. Complete recovery, including full physical activity, can typically be expected within four to six weeks. During the recovery period, our team provides comprehensive support and guidance to ensure a smooth and effective healing process.
4. What Happens if the Occipital Nerve is Cut?
Cutting the occipital nerve, known as occipital neurectomy, is generally considered only when other treatments and surgeries fail to relieve pain. This procedure involves severing the nerve to block pain signals. It is a more drastic measure and is not commonly performed because it can lead to numbness in the nerve’s area of sensation. Our approach focuses primarily on decompression to preserve nerve function while alleviating pain.
5. What are the Risks of Occipital Nerve Decompression Surgery?
As with any surgery, occipital decompression surgery carries some risks, which may include infection, bleeding, and potential worsening of headache symptoms, though this is exceedingly rare. There is also a small risk of damage to the occipital nerves, which can result in numbness or changes in sensation. We take meticulous steps to mitigate these risks, employing the latest surgical techniques and post-operative care practices.
6. Do You Need to Shave Your Head for Nerve Decompression Surgery?
No, it is not necessary to shave your head for occipital nerve surgery. Our surgeon typically require only a small area to be shaved where the incision is made, which is usually well-concealed by surrounding hair. We understand the personal and aesthetic concerns of our patients and strive to minimize the impact of surgery on appearance.
7. What Happens if Occipital Neuralgia Goes Untreated?
If left untreated, occipital neuralgia can lead to a persistent, debilitating pain that may worsen over time. Chronic pain can significantly impact quality of life, leading to difficulties in daily functioning, mood changes, and other health complications. Early and effective treatment, like occipital nerve decompression surgery, is crucial in preventing the progression of symptoms and improving overall well-being.
8. Why Choose Us for Occipital Neuralgia Surgery?
Choosing the right facility for your occipital neuralgia surgery is crucial. At Migraine Surgery Specialty Center, we are leaders in the field of headache and migraine surgery. Our team understands the complexities of nerve-related pain. We are dedicated to providing a compassionate and comprehensive treatment approach, ensuring that each patient’s individual needs are met with the utmost care and expertise.
Contact us for a further consultation

Living with the pain of occipital neuralgia can be challenging and isolating, but you don’t have to endure it alone. Our team at Migraine Surgery Specialty Center is here to help. If you or a loved one are suffering from symptoms of occipital neuralgia and are considering occipital nerve surgery, we invite you to contact us for a further consultation. Our goal is to provide relief and improve your quality of life through specialized, compassionate care. Reach out today to learn more about how occipital neuralgia surgery can help you regain control and live a pain-free life.
